
Tonsil and adenoid enlargement or infection
Causes:
Tonsils and adenoid enlargements in children may have intrinsic, unknown or infective origins.
Importance:
Adenoid and tonsil enlargement may result in blocked breathing passages, and snoring, which may be associated with reduced oxygen delivery to the brain and vital organs. Long term, it may contribute to reduced attention span and learning, bed-wetting, poor growth and weight control, reduced mandibular growth and poor dentition. Recurrent tonsillitis could be associated with sore throats, fevers, poor feeding, antibiotic resistance and absence from school/ work. Adenoid hypertrophy is often worse in children between 2 to 10 years of age. It also predisposes to chronic fluid in the middle ear (glue ear).

Investigations offered:
Examination in the clinic may include flexible nose endoscopy. X-ray evaluation if child cannot cooperate. Sleep study in complex cases – home or hospital based.

Treatment offered:
- Watchful waiting only if episodes are isolated, mild and without significant airway obstruction.
- Fever, pain and antibiotic medications
- Day surgery for tonsils removal may be required for chronic airway obstruction, severe or recurrent tonsillitis. Diathermy, radiofrequency and coblation methods are available.
Unclear speech
Causes:
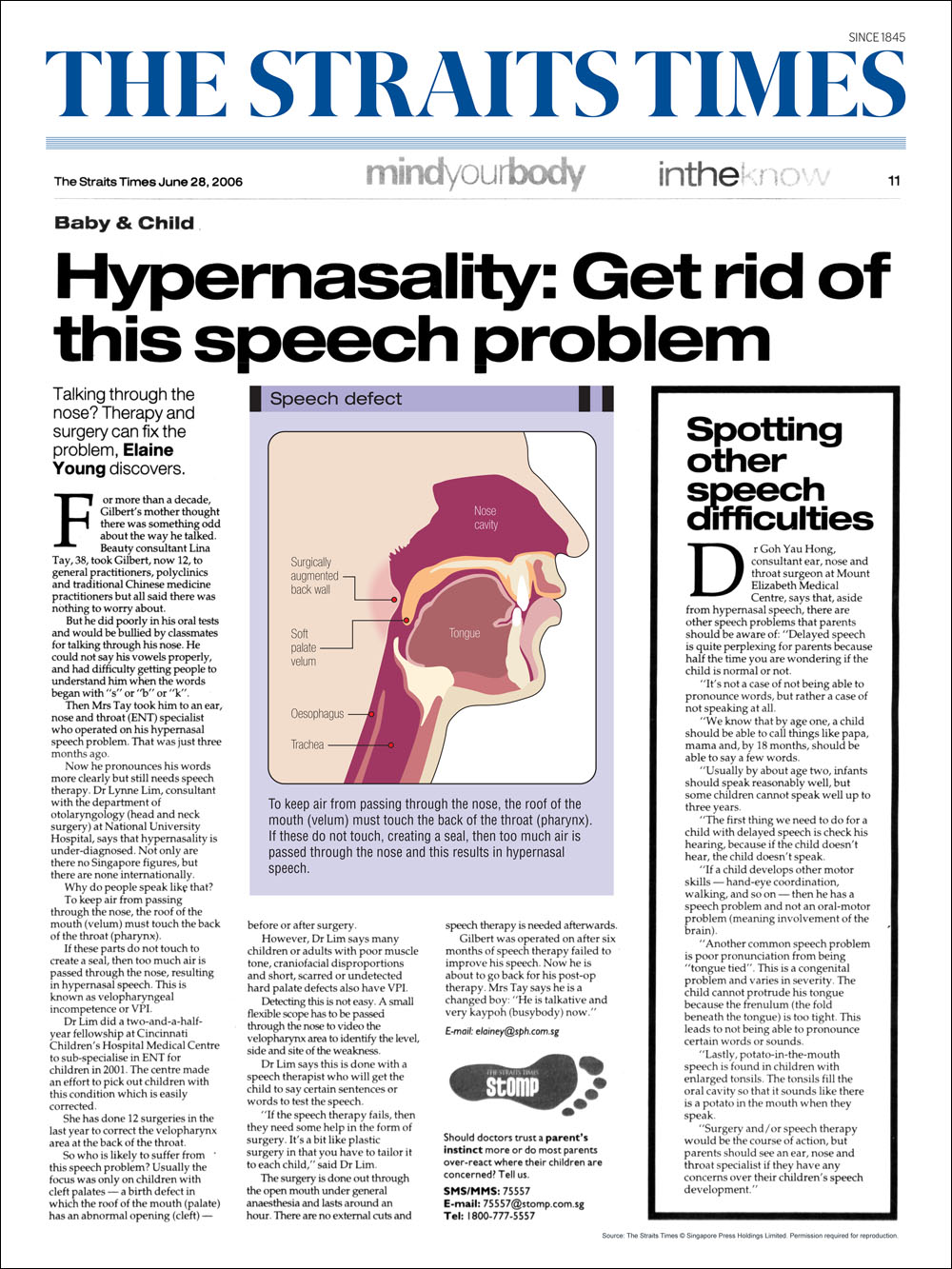
Can be due to tongue tie, oromotor poor coordination, wrong learning of speech, very large tonsils, cleft palate, submucous cleft, soft palate insufficiency/ weakness, disproportionate craniofacial structures, poor lateral pharyngeal wall tone, neurological disorders.(Read More: Hypernasality: Get Rid Of This Speech Problem)
Investigations offered:
- Examination of oral cavity with good headlight
- Flexible nasoendoscopy with patient speaking
- Work with a speech therapist/paediatrician/ plastic surgeon/ dental colleagues for multidisciplinary evaluation
Treatment offered:
- Tongue tie release if severe
- Work with speech therapy professionals
- Repair of submucous cleft, tonsillectomy, pharyngeal flap, sphincteroplasty as needed
Gastroesophageal Reflux Disease (GERD)
The ring of muscle between the esophagus and stomach is weak or relaxes abnormally. In Gastroesophageal reflux disease (GERD), backflow of the acid and non-acid stomach contents up into the voice box and laryngeal area causes irritation, phlegm and hoarseness in the throat. It is more common in children before the age of 1 year old. In more complex laryngeal and tracheal airway anomalies, it further narrows the airway via inflammation and swelling. Obesity, coughing, vomiting, straining or sudden physical exertion can also increase GERD.

Importance:
Gastroesophageal reflux disease GERD may not be associated with gastric pain or heartburn sensation. More often, it is just chronic throat irritation worse after meals or sleep, or hoarseness of voice that prompts an evaluation. It also worsens airway swelling in nose, throat and trachea in babies and young children, leading to noisy breathing. Children may have recurrent vomiting, crying, irritability and food refusals at meal times, with poor weight gain. GERD also increases the risk of chronic middle ear fluid and sorethroat.
Investigations:
- Nasolaryngoendoscopy in the clinic
- 24 hour double pH probe
- Barium swallow/ meal
- Evaluation by gastroenterology and swallow specialists
- Esophageal manometry or Pepsin test (for non-acid gastric reflux)
Treatment:
- Avoid bottle feeding lying down or near bed time
- Dietary and lifestyle modification: reduce weight, chocolate, peppermint, fried/ fatty foods
- Medication for reflux
- Refer to gastroenterologist for strangulated hiatal hernia or severe reflux

{kind=link}