
Head and Neck Lumps
Causes
Some common lumps
Salivary gland lumps – These could be benign or cancerous tumors, or swelling due to acute or chronic infections or stones blocking the salivary ducts. The main glands are the parotid, submandibular and sublingual glands.
Neck lymph nodes – These could be benign or cancerous nodes, and due to infections, systemic disorders and blood disorders. All nodes should be further evaluated if they are increasing in size and numbers, last more than 3 weeks, are fixed to the skin or ulcerate.
Thyroid lumps – These can be benign or cancerous, a Multinodular Goitre or generalised swelling eg in Grave’s Disease. May be associated with thyroid hormone disorders.
Thyroglossal cyst – This is a congenital cyst that is usually sited in the midline of the upper part of the neck, and moves with swallowing. Cancerous change is possible but rare.
Branchial cyst – This is a congenital cyst that is usually sited at the upper half of the lateral neck.
Ranula – This usually presents as a floor of the mouth and sometimes below the chin soft cystic swelling. Due to the trapping of salivary mucus.
Rarer lumps include:
- Hemangioma and Lymphangioma – These are vascular and lymphatic malformations, filled with blood or lymphatic fluid.
- First branchial cysts/ sinuses – These present as lumps/ openings around the ear region or angle of the jaw. The sinus tract is often complexly related to facial nerve and vessels in the head and neck.
- Parathyroid, neck nerve and vessel tumors
Importance
Besides presenting as a lump, head and neck tumors may present as blood stained sputum, nose bleed, hearing loss, ringing in the ear and ear block. The lumps may swell with infections and reduce in size in between episodes. Destruction of structures closely related in the head and neck region results in various problems with breathing, swallowing, eating, voice, dentition, cosmesis and bleeding. Seeking evaluation and treatment as early as possible is critical for ensuring the best outcomes for cancer cases
Investigations
- Blood tests for screening of some cancers like nasopharyngeal carcinoma (NPC), especially with family history of NPC
- Blood tests for blood disorders
- Fine needle aspiration cytology (FNAC) in the clinic to differentiate benign and cancer pathology, with or without ultrasound guidance
- Ultrasound scans are useful for neck lumps to determine size, numbers, and suggest if the tumor is likely to be benign or cancerous.
- Excision biopsy under local or general anaesthesia for definitive histopathology and diagnosis
- CT scan, MRI scans to determine complexity of anatomy, extent of disease, spread and recurrence
Treatments
- Excision of the lump tailored to specific diagnosis. For non-cancer lumps, the prognosis is good and there is significantly less risk to other structures in the head and neck
- For cancer lumps that are not discovered early or contained, surrounding head and neck structures often need to be removed enbloc to reduce the risk of recurrence. Where possible, efforts are made to preserve important structures to allow for swallowing, voice, breathing without a tracheotomy and cosmesis
- Various chemotherapy and radiotherapy options may be required additionally, for optimal tumor clearance and to reduce the risk of recurrence
Hoarse voice
Causes
Most commonly due to infection, haemorrhage into or allergic reaction of the vocal cords (voice box) if of sudden onset. May be from excessive strenuous voice use, smoking, hypothyroidism and drugs leading to polyps, cysts and nodules. May be cancer change in the larynx or invasion from surrounding thyroid or other neck region tumors. Trauma to the larynx may dislocate the laryngeal cartilages. Post surgery or radiation therapy for cancer or tumors in the head and neck and pathology in the chest.(Read More: Listen To Your Voice)
Importance
The voice may become raspy, harsh, of different pitch and low volume. Hoarseness lasting more than 3 weeks requires evaluation to exclude more sinister causes.
Investigations offered
- Throat examination
- Flexible nasolaryngoendoscopy in the clinic with patient voicing
- Biopsy via endoscopic non-open methods under general anesthesia (Endoscopic Laryngeal Microscopic Surgery)
- CT scan and MRI radiology of the base of skull, neck and chest
Treatments offered
- Observation for spontaneous recovery in acute infections.
- Voice rest. Avoid voice overuse of wrong use. Voice training and rehabilitation by speech and swallow therapist.
- Stop smoking. Better control of gastroesophageal reflux (eg avoid spicy, sour and oily food and caffeine).
- Medications for cough, gastroesophageal reflux and allergies as appropriate.
- Surgery for benign nodules, cysts and polyps
- Surgery for trauma to the larynx/ vocal cords
- Surgery for cancer of the larynx would require further investigations for extent of involvement and spread. Endoscopic, laser or open surgery, with or without chemotherapy and radiation therapy.
Feeding/ Swallowing Disorder
Causes
The problems can affect the oral, pharyngeal or esophageal phase.
Due to poor dentition, neurological conditions (eg stroke, vocal cord, brain and spinal cord injury, Parkinson’s disease, sclerosis, Alzheimer’s disease) and head and neck pathologies (mouth, throat, esophagus cancers, injury and surgery).
Importance
There may be coughing/ gurgling/ increased effort and time/ drooling when eating and drinking. There may be recurrent lung infections from aspiration, weight loss and dehydration.
Investigations
- Work with gastroenterologists, swallow pathologists, physiotherapists.
- Observe feeding to see the patient’s posture, behavior, and oral movements during eating and drinking.
- Modified barium swallow
- Swallowing process viewed on X-ray (Videofluoroscopy)
- Nasolaryngoendoscopy when patient feeds for phase and types of food affected
Treatments
- Medication for acid reflux
- Address the underlying cause
- Swallow therapy to improve feeding coordination and acceptance of different food
- Direct feeding therapy designed to meet individual needs, eg postural changes
- Nutritional changes (optimize calories and types of food)
Stridor
Causes
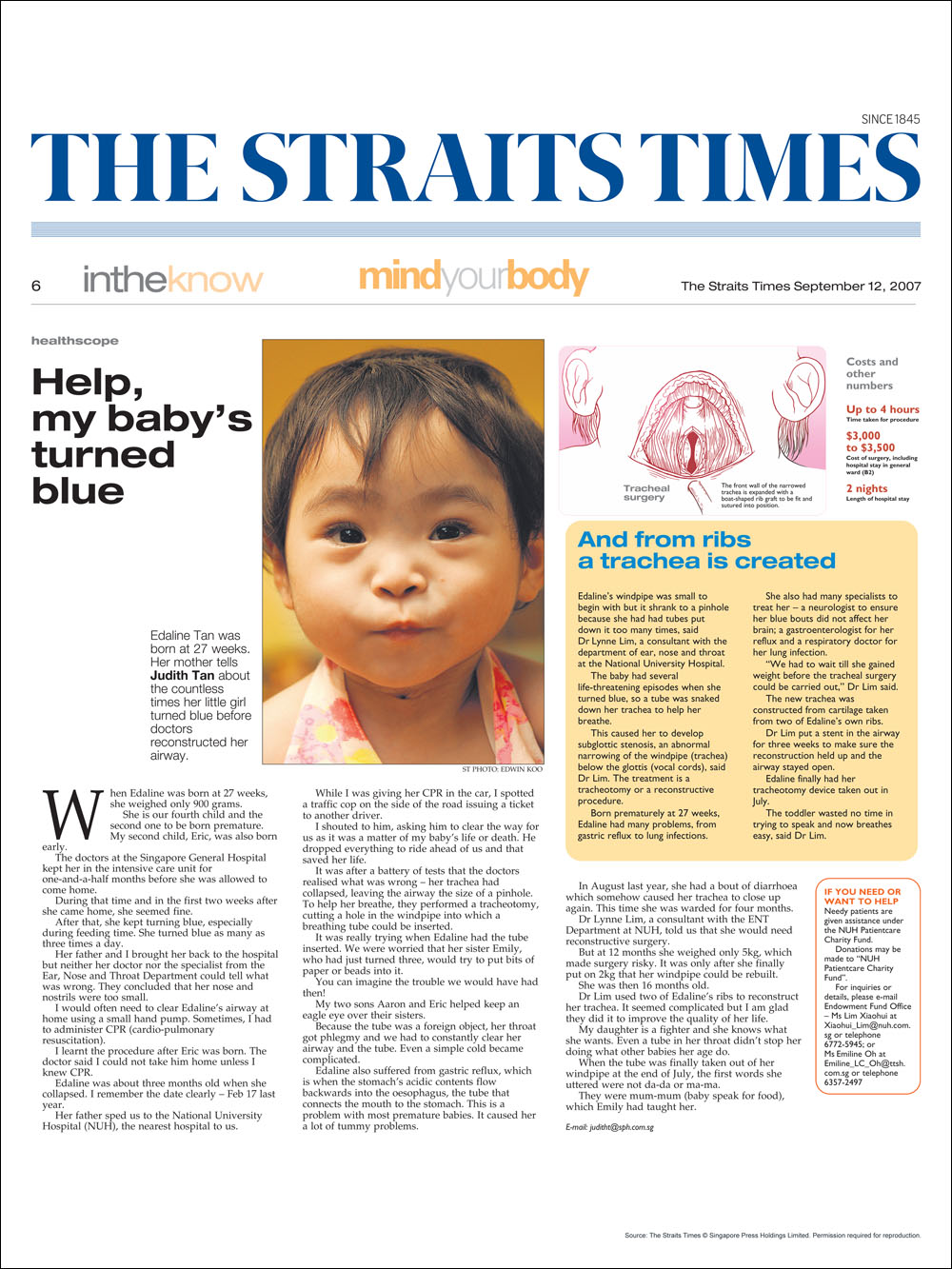
Include tumor, papillomatosis of the larynx and trachea, compression of the trachea by neck masses like thyroid lumps, base of skull tumors affecting the vagal nerve, strokes, vagal nerve pathology that impair mobility of the vocal cords, swelling and inflammation of the vocal cords due to infection, chemotherapy, drugs, trauma and idiopathic causes.(Read More: Help, My Baby’s Turned Blue)
Importance
Stridor is noisy breathing arising from blocked airway at the level of the voice box and trachea. When significant, there is risk of acute oxygen lack, respiratory distress leading to cardiac arrest and death. Feeding, swallowing, voice and lung function are often concurrently affected.
Investigations
- Nasolaryngoendoscopy in the clinic
- Xray neck, Chest Xray, CT scan and MRI
- Microlaryngobronchoscopy (MLB) under GA to evaluate the lower trachea and lung airways, and for biopsy
- Feeding and swallowing evaluation
- Voice evaluation
- Lung function evaluation
Treatment
- Emergency medications
- Emergency intubation with ICU care
- Surgical tracheotomy
- Treatment tailored to the underlying cause (eg laser or microdebrider removal of papillomatosis, lateralisation of the vocal cords, repositioning of acute dislocation of vocal cord cartilages, cardiothoracic surgery for cardiac and thoracic trachea pathology)
- In subglottic stenosis and trachea involvement, balloon dilatation, plastic and wire stents, anterior and posterior rib graft trachea reconstruction, cricotracheal resection, segmental trachea resection and tracheoplasty are some options available to avoid permanent tracheotomy
- In cancers of the larynx, preservation techniques for voice and swallowing is attempted where possible.

{kind=link}