
A. Head and neck lumps
Causes:
The most common lumps are neck lymph nodes swelling from infections and congenital thyroglossal and branchial cysts. Other lumps are vascular lesions, lymphangiomas, salivary gland (parotid, thyroid and sublingual) and floor of mouth lesions. Cancers are less common in children, with many malignancies being blood cell origin.
Importance:
Lymph nodes more than 2 cm diameter, rubbery, enlarging or fixed require further evaluation. Repeated infections, pain, discharge is possible. Swallowing and voice may sometimes be affected. Malignancies though rarer must be excluded.
Investigations:
- Clinic examination and palpation may need to be supplemented with flexible nasolaryngoscopy of the upper airway
- Ultrasound scans of the neck and superficial lumps
- Fine needle aspiration cytology to differentiate benign and cancer lumps
- CT or MRI scan
Treatments offered:
- Medication (oral, injectable) for infections, hemangioma, lymphangioma
- Surgical excision for bioipsy, noresolving lumps and for definitive diagnosis
- Lymphangiomas and vascular hemangiomas can be particularly challenging with infiltration between important head and neck regions harboring key vessels and structures, with higher risk of residual and recurrent disease
B. Hoarseness
Causes:
In young children, chronic hoarseness is usually due to voice abuse and screaming resulting in vocal cord nodules and hemorrhage. It can be aggravated by laryngoesophageal reflux disease. Other causes are trauma, respiratory papillomas, post intubation and post surgery for pathology in the chest, head and neck.(Read More: Listen To Your Voice)
Importance:
The voice may become raspy, harsh, of different pitch and low volume.
Investigations offered:
- Throat examination
- Flexible nasolaryngoendoscopy with patient voicing
- Biopsy via endoscopic non-open methods under general anesthesia (Endoscopic Laryngeal Microscopic Surgery)
- CT scan and MRI radiology of the base of skull, neck and chest
Treatments offered:
- Observation for spontaneous recovery in acute infections.
- Voice rest. Avoid voice overuse of wrong use. Voice training and rehabilitation by speech and swallow therapist
- Better control of gastroesophageal reflux
- Control of cough, gastroesophageal reflux and allergies
- Endoscopic minimally invasive surgery for benign nodules, cysts, and polyps
- Endoscopic or open neck surgery for trauma to the larynx or vocal cords
C. Feeding/ Swallowing Disorder
- Problems gathering food and sucking, chewing, or swallowing it
- Due to reflux, metabolic, nervous system disorders (e.g., cerebral palsy, meningitis, encephalopathy), prematurity and/or low birth weight, airway conditions, laryngeal cleft, vocal cord palsy, laryngoesophageal fistula, heart and lung disease, cleft lip and/or palate, muscle weakness
- Easily missed with unusual signs during feeding: arching or stiffening of the body/ irritability/ coughing or gagging/ refusing food or liquid/ only wants certain types of foods eg pureed/ long feeding times/ difficulty chewing
- Other signs are: drooling or food coming out of the mouth or nose/ difficulty breathing when feeding/ gurgly or hoarse voice, frequent vomiting/ recurrent lung infections/ poor weight gain
Multidisciplinary consults with pediatricians, gastroenterologists, speech-language swallow pathologists, physiotherapists.
- Observe patient’s posture, behaviour, and oral movements during feeding
- Modified barium swallow
- Swallow process is viewed on an X-ray (Videofluoroscopy)
- Nasolaryngoendoscopy when patient feeds with different foods
- Medication for acid reflux
- Address the underlying cause
- Swallow therapy to improve feeding coordination and acceptance of different food
- Individualised direct feeding therapy
- Nutritional changes (optimize calories and types of food)
D. Stridor
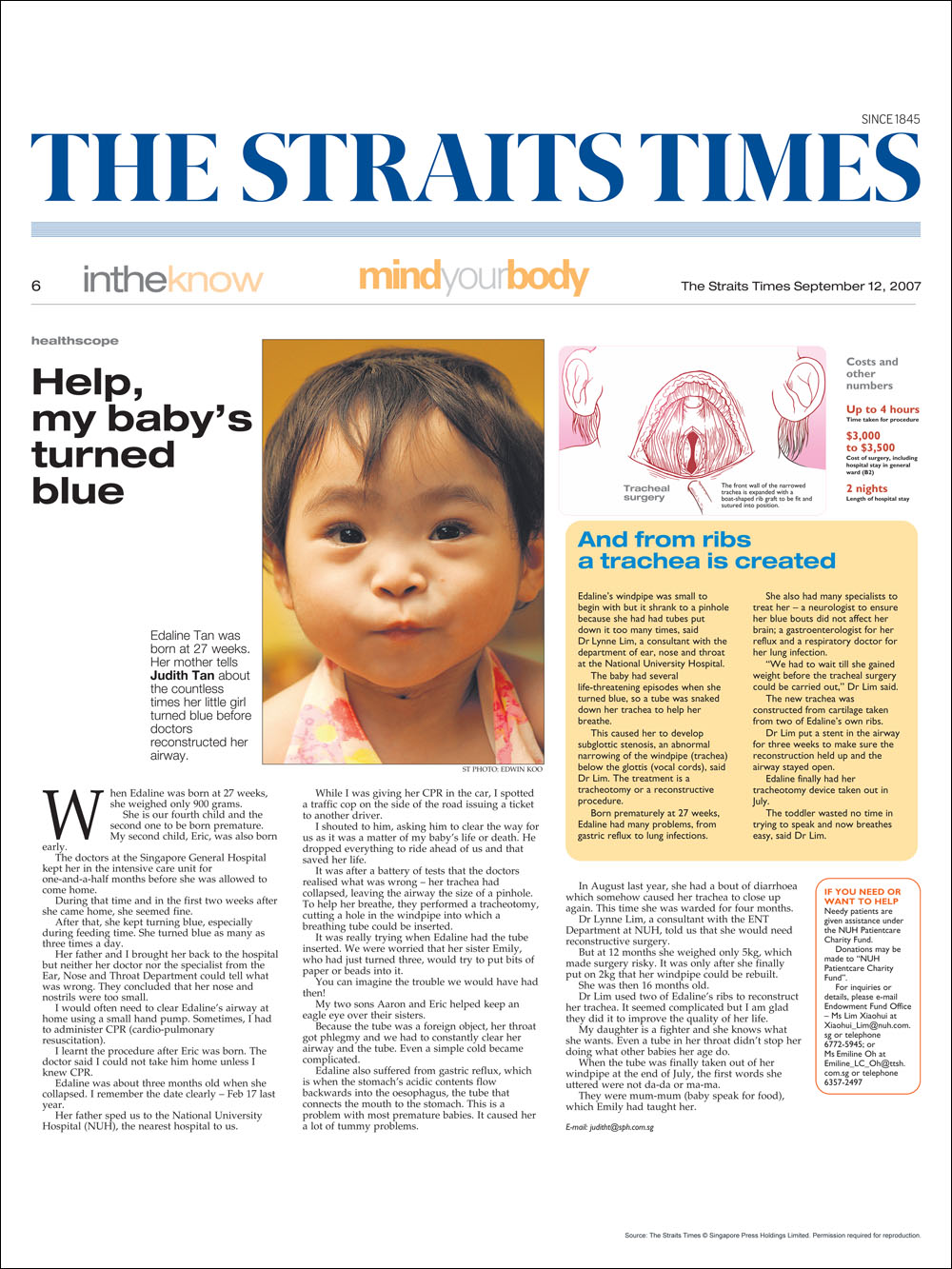
Stridor is the sound arising from blocked vocal cord or trachea sites airway obstruction, and different from stertor arising from nose block or wheezing from bronchial airway block. A specialized multidisciplinary medical, surgical, therapist, anaesthetist and HD/ ICU team carefully coordinating the care is a must. In young children especially, the condition may be associated with complex and multiple system issues and the oxygen reserve is tenuous.(Read More: Help! My Baby’s Turned Blue)
Stridor is the sound arising from blocked vocal cord or trachea sites airway obstruction, and different from stertor arising from nose block or wheezing from bronchial airway block. A specialized multidisciplinary medical, surgical, therapist, anaesthetist and HD/ ICU team carefully coordinating the care is a must. In young children especially, the condition may be associated with complex and multiple system issues and the oxygen reserve is tenuous.(Read More: Help! My Baby’s Turned Blue)
Causes:
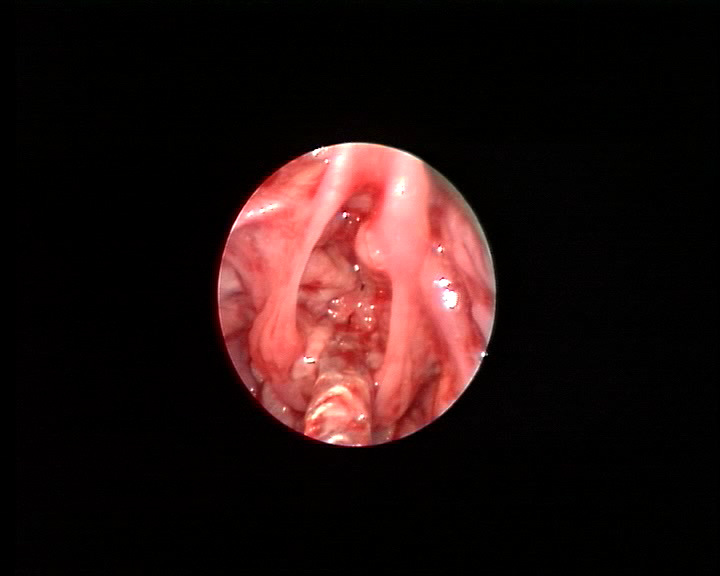
Photo 37 laryngeal lymphangiomaUsually include inhaled or swallowed foreign body obstruction, prolonged intubation with subglottic stenosis, laryngomalacia, congenital airway anomalies which are often complex, vocal cord palsy, hemangioma and lymphangioma, epiglottis infection, recurrent respiratory papillomatosis and vagal nerve injury from chest surgeries. Congenital cases may have heart and chest vasculature anomalies.
Causes:
Photo 37 laryngeal lymphangiomaUsually include inhaled or swallowed foreign body obstruction, prolonged intubation with subglottic stenosis, laryngomalacia, congenital airway anomalies which are often complex, vocal cord palsy, hemangioma and lymphangioma, epiglottis infection, recurrent respiratory papillomatosis and vagal nerve injury from chest surgeries. Congenital cases may have heart and chest vasculature anomalies.
Importance:
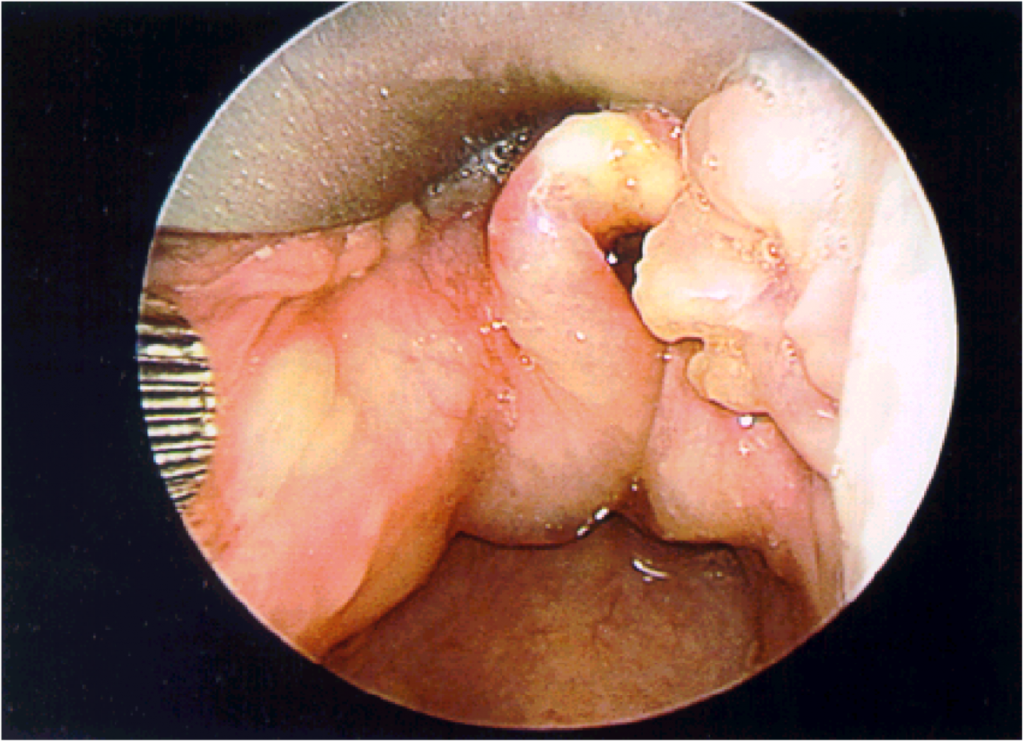
Photo 38 laryngomalaciaStridor is noisy breathing arising from blocked airway at the level of the voice box and trachea. There is risk of acute oxygen lack, respiratory distress, cardiac arrest and death. Feeding, swallowing, voice and lung function are often affected.
Importance:
Photo 38 laryngomalaciaStridor is noisy breathing arising from blocked airway at the level of the voice box and trachea. There is risk of acute oxygen lack, respiratory distress, cardiac arrest and death. Feeding, swallowing, voice and lung function are often affected.

Investigations:
- Nasolaryngoendoscopy in the clinic
- Xray neck and chest, CT scan and MRI
- Microlaryngobronchoscopy (MLB) to evaluate tracheobronchial airway and biopsy
- Feeding, swallowing, voice and lung function evaluation
Treatment:
- Emergency medications or intubation for swelling of vocal cords
- Surgical tracheotomy (limits learning, work, social options, risk of dislodgement and blockage, 24 hour care needed)
- Treatment tailored to the underlying cause (eg laser or microdebrider removal of papillomatosis, lateralisation of vocal cords, repositioning of dislocated vocal cartilages, cardiothoracic surgery)
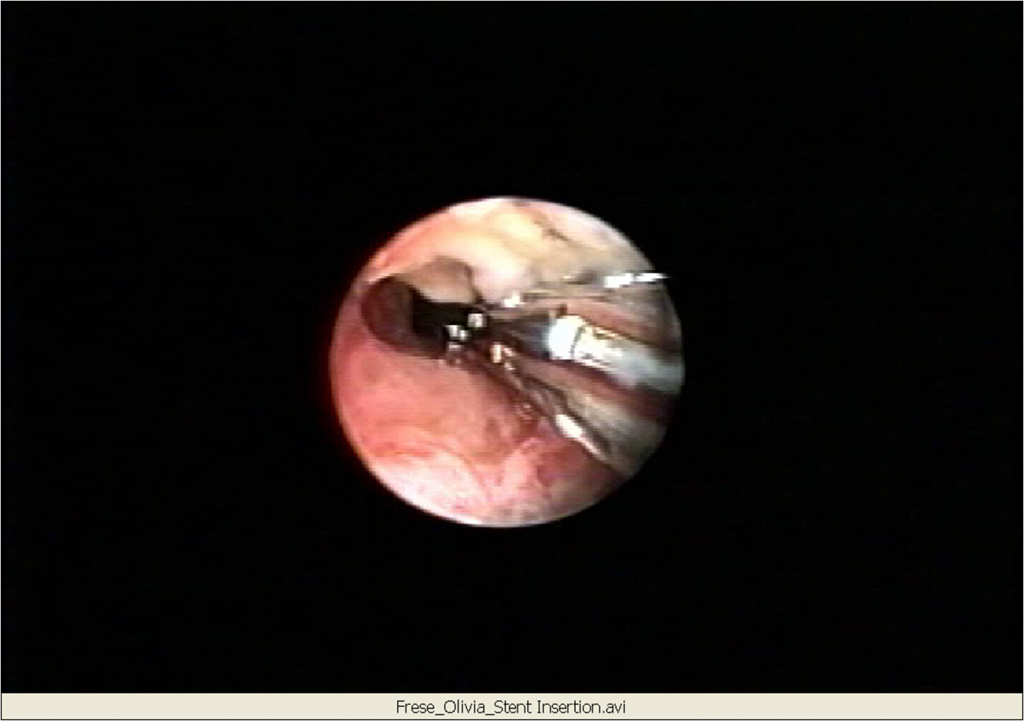
- In subglottic/ trachea stenosis, balloon dilatation, plastic and wire stents, anterior and posterior rib graft trachea reconstruction, cricotracheal resection, segmental trachea resection and tracheoplasty options to avoid permanent tracheotomy

")

{kind=link}